


Genetics

In this section, I will provide a brief introduction to psychiatric genetics. It's a vast field, so this will only be a short overview. A research colleague,
, writes many very readable articles on psychiatric genetics. I recommend reading his work if you're interested.Family Ties: Heritability
Genetics is based on the observation that many psychiatric patients have parents or other family members who are also affected. Sometimes, both children and parents are seen at the same clinic. A classic Swedish study from the Karolinska Institute investigated how bipolar disorder and schizophrenia co-occur in families.
Classical genetics is based on observations by Gregor Mendel in the 19th century, where he could track how hereditary traits in plants evolved in the garden. Of course, he did not know the mechanism behind it, like the structure of the genetic material and how it is passed on through generations. Despite this, he, along with others, provided us with an understanding of how different traits work. Psychiatric disorders, however, are much more complicated and are governed by a large number (likely thousands) of genes, as opposed to simpler phenotypes like eye color. To study heritability in humans, researchers examine twins (both identical and fraternal), siblings, and sometimes adopted children. For example, by comparing how common it is for identical twins to have a particular disease compared to fraternal twins, you can estimate how much of the variance is explained by genetic factors. This is known as heritability. The figure below is from Abdel Abdellaoui and shows the heritability of various psychiatric disorders.
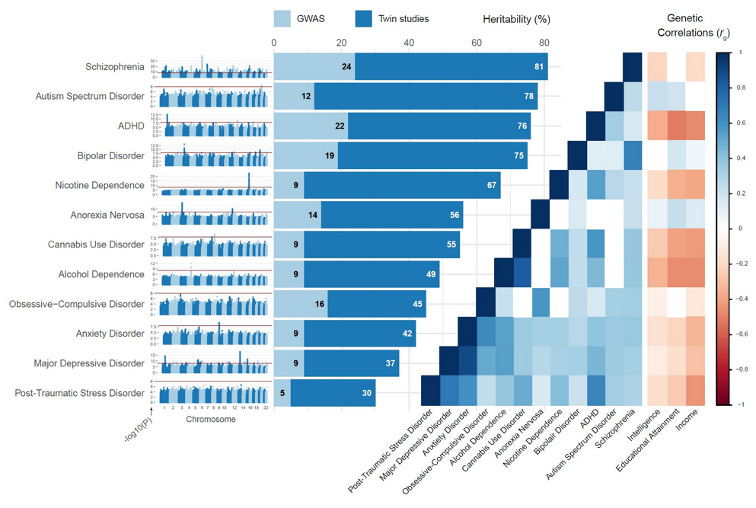
As you can see, the heritability for schizophrenia is 81%, and for bipolar disorder, it's 75%. Once it was realized how heritable these conditions are, worldwide consortia have collected samples from thousands of patients to find the gene variants that explain the variance (Psychiatric Genomics Consortium, PGC). They have searched for common variants in the genome where one base is substituted for another (single nucleotide polymorphisms, SNP). This is a natural variation that all humans have, but some are associated with disease risk. Each variant only leads to a small increased risk, but the logic is that with many risk variants, you eventually end up at risk for the disease. These studies are called genome-wide association studies (GWAS in the figure above refers to how much of the heritability is explained by single nucleotide polymorphisms). In the case of schizophrenia, there are also clearly more rare gene variants (ultra-rare) and even larger chromosomal changes (copy number variations, CNV) that greatly increase the risk of the disease. The image below shows these three groups of risk genes: their frequency (x-axis) and how much they increase the risk of schizophrenia (y-axis). See the original article here.

Single nucleotide polymorphisms are the blue ones and are clearly weaker risk factors than the more rare ones (yellow and red). For bipolar disorder, not as many rare variants have been found, nor CNVs.
Polygenic Risks
But how do you account for whether a person has multiple risk variants but not all of them? One way is to add up the variants you have, both considering whether you have both alleles and how much the risk increases (odds ratio, OR). You could simplify it as follows, where PRS stands for polygenic risk and N is the number of alleles (0, 1, or 2).
PRS = OR1 * N1 + OR2 * N2 + ... + ORn * Nn
The number of risk variants included (n above) depends on various statistical considerations. After further normalization of PRS, a value can be assigned to all individuals that describes their total genetic risk for a particular disease (risk from SNPs). It's important to remember that this applies not only to patients but to everyone. For example, you can calculate the genetic risk for bipolar disorder or schizophrenia for a completely healthy person. When normalizing PRS, it's usually seen as a normal distribution with a mean of 0. Thus, the vast majority of individuals have low risk (around 0), but a smaller and smaller number have higher (and lower) risk. The image below comes from Wikipedia, and on the left, you can see the normal distribution.
This was a brief introduction to psychiatric genetics. There is so much more to explore if you're interested. In later sections, I plan to write more about how to analyze the distribution of different genetic structures among psychiatric patients and how to understand how risk genes can lead to disease.